by Linda Rawson | Oct 14, 2019 | Industrial Hygiene
For some situations, like office work, the primary safety hazard might be a paper cut. In industrial professions, employee safety is at risk every day. Because of legalization of marijuana, industrial accidents could occur more often because marijuana can impair an employee’s coordination and motor skills.
Where is Marijuana Legal Right Now
Despite many states legalizing cannabis in the United States, marijuana remains an illegal drug according to the federal government. The government classifies cannabis or marijuana as a Schedule I drug. Schedule I drugs, under the federal Controlled Substances Act (CSA), are those drugs that possess a high potential for abuse and for which there is no currently accepted medical use. The DEA reviewed its classification of marijuana in 2016, and affirmatively chose to keep marijuana on the list Schedule I drugs.
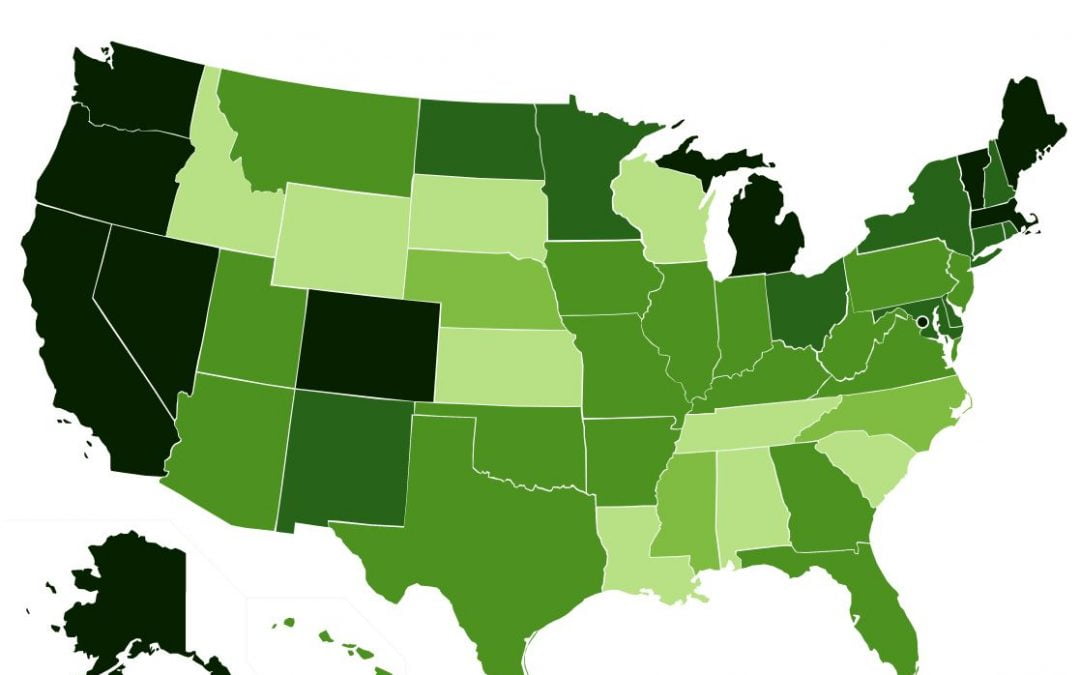
A nice map from DISA Global Solutions shows the marijuana legality by state with links to the state law.

Map of Marijuana by State
How is Marijuana Use Impacting Safety on the Job?
People try marijuana to get “high.” The psychoactive ingredient, tetrahydrocannabinol (THC) in marijuana stimulates the brain to produce dopamine which relaxes the body. According to an article by WebMD, How Marijuana Affects Your Mind and Body, affects sensory perception (brighter colors, louder sounds), reaction time, motor skills, and increase risky behavior. For an employee working in an industrial environment, operating machinery, or driving industrial equipment, these effects can be deadly.
According to a study, How does marijuana use affect school, work, and social life?, by the National Institute on Drug Abuse (NIDA), 55 percent more workplace accidents, 85 percent more injuries at work, and 75 percent more absenteeism when an employee tested positive for cannabis.
The Employer Usually Wins a Lawsuit
As a result of cannabis use, an employee’s job is terminated. When this happens states typically side with the employer even if the employee has a medical marijuana card. However, marijuana is still Schedule I drug which is illegal according to federal law. Federal law supersedes state law.
- The Americans with Disabilities Act sides with the employer when it comes to medical marijuana use
- If an industrial accident occurs and a worker is injured, worker compensation is not provided if an employee was under the influence
- Most health insurance programs do not cover medical cannabis as part of their list of prescription drugs
What Makes a Good Drug Policy?
An interesting study on the impact of Drug-Testing programs by the National Center of Biotechnology Information (NCBI) shows the effective use of pre-employment drug testing concludes it is useful to employers choosing job applicants. An employer drug policy should include:
- Management training to ensure enforcement the drug policy
- Employee support options including company assistance or local resources
- Clearly defined use and possession guidelines
- Criteria for post-accident analysis
- Rules employee’s conviction or arrest for drugs
Legal authorities review drug policies and workplace procedures to ensure reduction of litigation by employee. Policies may change based on state or even federal law and could change frequently. The drug policy should have a date and acknowledgment by the employee. By having this information, litigation against the employer is protected.

Cannabis picture by pixabay
The health and safety of your workforce depend upon you to keep them safe.
Linda Rawson, is the Founder of DynaGrace Enterprises, inventor of WeatherEgg, and the author of The Minority and Women-Owned Small Business Guide to Government Contracts: Everything You Need to Know to Get Started

by Linda Rawson | Apr 13, 2019 | Air Quality
Throughout history, air pollution has been a problem. Not only smog but fumes from excessive coal use in households as well as dirty air released from manufacturing, mining and increased emissions from industrial processes. Respirators were invented.
Londoners even coined a phrase, “pea-soupers,” because, since the 14th Century, London has been affected by thick smog.
Because of poor air, civilizations learned to deal with air pollution by using respirators of different types whether basic or technologically advanced.
![Pliny the Elder, Library of Congress [Public domain]](https://upload.wikimedia.org/wikipedia/commons/4/49/Pliny_the_Elder.png)
Pliny the Elder, Library of Congress [Public domain]
In the 16th century, Leonardo da Vinci proposed using a woven cloth dipped in water over the face to protect against the toxic chemicals used in chemical warfare.
Expanding on the need for protection of the industrial worker’s lungs, inventors offered other solutions in the centuries that followed.
In 1849, Lewis Phectic Haslett invented the “Lung Protector” which allowed a mouthpiece fitted with two clapper valves and used a wool filter to keep out dust. The first U.S. patent, US 6529, for a “Lung Protector” was recorded in 1849 and was for a respirator that utilized one-way valves moistened with sheep wool to filter dust.
In 1860, A Scottish chemist, John Stenhouse, decided to use charcoal in a wide variety of air-purifying devices. He invented the first respirator that captured toxic gases from the air. He especially wanted to protect firemen and first responders.

John Stenhouse Mask, Public Domain
As even more, innovative scientific minds gained interest in air purifying devices, a race occurred to develop respirators that could protect against a broader range of air pollutants, such as hazardous gases.
In 1871, British physicist John Tyndall took Stenhouse’s mask, added a filter of cotton wool saturated with lime, glycerin, and charcoal, and invented a “fireman’s respirator,” a hood that filtered smoke and gas from air. Mr. Tyndall exhibited this respirator at a meeting of the Royal Society in London in 1874.
Also in 1874, Samuel Barton patented a device that ‘permitted respiration in places where the atmosphere is charged with noxious gases, or vapors, smoke, or other impurities.’ The first to include rubber and a metal hood structure, the Samuel Barton Respirator had a filter located in front and two eyepieces made of glass. The metal canister design contained lime, glycerin-soaked cotton wool, and charcoal.

Haslett Gas Mask, Frogstorm
In 1879, Hutson Hurd’s design improved on the design of the Haslett Lung protector and invented the design of the cup-shaped mask. The Hutson Hurd’s H.S. Cover Company manufactured these cup-shaped masks well into the 1970s.
Respirator Inventions World War I
After World War I, the military became much more involved and developed an intense interest in the use of respirators primarily as a defense mechanism against chemical warfare. Because of the military interest and money, the advances in the creation of inexpensive, useful filters increased in the 1930s. The filters were initially made with resin-infused dust and were further developed using fine particulates of glass fiber that could eliminate particulate matter. The design of the filter helped with the breathing ability that was not inhibited by the filters.
Post World War I
After World War I, the United States and the United Kingdom faced some of the worst air pollution cases in history.
In 1943, Los Angeles, California (LA), long known for its poor air quality, suffered from its first smog incident. LA’s factories and massive vehicle industry were to blame for the smog.

Nelson’s Column during the Great Smog of 1952
In December of 1952, the “great smog” or “big smoke” caused the city of Long to be engulfed in a thick layer of air smog which lasted for five days and resulted in 12,000 plus fatalities and 100,000 reported cases of respiratory illness. The smog was caused by the cold weather, lack of wind and the subsequent use of too much coal to heat the country.
In 1965, the Army provided an Emergency Respirator that consisted of Lucite, machined channels and a cover place that was secured by screws or adhesive. The mask did not have any moving parts but did have an amplifier that air could flow through. The technology was developed by the Harry Diamond Laboratories which later became part of the United States Army Research Laboratory.
The Future of Respirators
According to the World Health Organization, the top three of most air-polluted cities in the word rated by Particulate Matter (PM) concentration are 1) Kanpur, India, 2) Faridabad, India, and 3) Gaya, India. Other countries have issues including Pakistan, Uganda, China, and Qatar. Global air pollution problems and continuing climate change will put pressure on developing countries and will allow more advancements in the use of respirators.
The bigger the monetary fine, the more public health exposure, the more advancement of air pollution initiatives will continue. Labor laws, like the OSHA’s Respirable Crystalline Silica Standard standard for both Construction and General Industry, will become more refined to help protect workers. Because of the laws, respirators will continue to advance technologically.
Respirator technology is becoming sleeker, and most people wear primitive forms of respirators, like surgical masks, for protection. Surgical masks only work for airborne viruses and not air pollutants. In Japan, young people have used surgical masks as a fashion accessory to not only cover the face but protect from airborne viruses.
The human factor of respirators of the future will depend on comfortable fit, the mood of the wearer, and the actual protection the respirator provides, especially in an industrial environment.
The need for raising awareness of protecting your lungs from air pollution continues to be profound. Surgical masks will not work to eliminate PM, and in industrial situations, specific processes should always have the employee where a respirator mask.
To learn more about DynaGrace Enterprises mission for Helping People Breathe Cleaner Air visit this page -> https://dynagrace.com/capabilities/air-quality/

by Linda Rawson | Feb 22, 2019 | Industrial Hygiene

Two male industrial workers who were inside a West Virginia ceramics factory, Public Domain Picture by CDC
From the day we’re born, taking a deep breath is something we all take for granted. Silica in an industrial environment is common place.
Adults breathe 12 – 20 times a minute when they are resting.
As humans, we take between 17,000 – 30,000 breaths a day, and the total length of the airways in our lungs is estimated to be 1491 miles (2,400 km.) The equivalent of Denver, Colorado to New York City, NY in travel! However, every breath you take has the potential to cause silicosis. Especially if you work in an environment where you are exposed to respirable crystalline silica (RCS).
What is silica?
Silica is a fundamental component of soil, sand, granite and many other minerals and is found in many places on Earth. The most common form of silica is Quartz (the other two have cristobalite and tridymite). All three forms create breathable particles when workers chip, cut, drill or grind objects containing silica.
Related article: OSHA Publishes Silica Standard FAQ
Silica, is a primary component of the Earth’s crust, is present in a wide range of industrial and non-industrial environments and consumer products (including many cosmetics and cat litter).
The breathing of the silica dust generated from these activities can have a devastating effect on health, which can cause lung cancer and silicosis.
When we talk about the dangers of silica, the word “silicosis” immediately comes to mind.
Silicosis itself tends to be linked to mining. The weakening lung disease, caused by the inhalation of crystalline silica dust, has flourished in medical, political and social policy responses and has captured the public imagination expressed in popular culture, from mining ballads to representative art.
There are legitimate reasons for this – not least the massive harm to the lungs caused by the disease. Silicosis has precedence of being a dangerous occupational disease and has made its mark in the mining industry in the global economy.
However, when it comes to silicosis, the mining industry is not the full story, and silicosis is not the primary disease when it comes to silica risks.
Since the 1990s, medical science has re-evaluated the potential role of silica in triggering inflammatory diseases, autoimmune diseases which include systemic lupus erythematosus, scleroderma, rheumatoid arthritis, and sarcoidosis. Although it was previously thought to be harmful only when inhaled in the form of dust, the question now arises whether exposure to silica in other forms can also be risky.
The road from safety to occupational health, industrial hygiene and well-being may be a long and winding road, but as practitioners, we get the hierarchy of control measures. If we all took the time to consider RCS and whether our existing control measures were designed to ensure routine maintenance and control of RCS, we would each contribute to reducing the number of people dying of silicosis and keep the worker safe.
References:
https://rospaworkplacesafety.com/2016/06/29/every-breath-you-take-a-brief-history-of-silica-and-silicosis/
http://www.sciencespo.fr/silicosis/content/silica-and-silicosis-history

by Linda Rawson | Feb 11, 2019 | Industrial Hygiene
OSHA put out a Request for Information (RFI) to ask for additional information regarding the respirable crystalline silica standard. OSHA revised the silica standard March 25, 2016, and launched an industry compliance effort on September 23, 2017, with full enforcement of the October 23, 2017 standard.

The U.S. Army Corps of Engineers working on Folsom Damn. Photo allowed from Public Domain by US.
The 2016 OSHA rule lowered the Permissible Exposure Limit (PEL) to 50 micrograms per cubic meter (µg/m3) of air as an 8-hour Time Weighted Average (TWA) in general industries. OSHA considers that level to be technically achievable for affected industries. In construction, OSHA put an Action Level (AL) of 25 µg/m3 over 8-hour TWA, among other requirements. The original OSHA standard established in 1971 had a PEL of 250 µg/m3 in the construction industry and 100 µg/m3 in general industry.
Related article: OSHA Publishes Silica Standard FAQ
The OSHA standard for the construction industry is strict, and the criteria are listed in Appendix I: OSHA Respirable Crystalline Silica Standard for Construction. Inside the appendix is a table of engineering controls, work practices, and respiratory protection specified for everyday construction job tasks that possibly release respirable crystalline silica. Employers that comply with the methods defined in “Table 1– Specified Exposure Control Methods When Working with Materials Containing Crystalline Silica ” are exempt from the PEL or demands for monitoring of employee worker direct exposures. However, employers should be willing to protect workers.
OSHA Seeking Additional Information
OSHA has issued the RFI to solicit comments from industry on Table 1. OSHA described its plan in the Fall 2018 schedule of governing and deregulatory actions. Regarding the Fall of 2018 agenda, OSHA said it had an interest in 3 details:
- The efficiency of control determines not consisted of for tools and jobs listed in Table 1;
- Tasks and even devices including exposure to respirable crystalline silica that is not noted in Table 1; and
- The performance of dirt control methods in limiting employee exposures to respirable crystalline silica when executing those procedures.
In evaluating the responses to the RFI, OSHA will determine if alterations to Table 1 are ideal and needed.
Lower PEL Full of Controversy
Regarding the OSHA 2016 rule, the development of lower PEL was subject to controversy, debatable and probably would be challenged in federal court.
Nevertheless, December 22, 2017, the three-judge panel of the UNITED STATES Court of Appeals in Washington DC upheld the OSHA rulemaking with one exception, finishing a challenge by North America’s Building Trades Union and US Chamber of Commerce. An agreement was made that OSHA’s medical removal requirements were arbitrary and instructed the agency to reconsider them.
What Should Employers Be Aware Of?
Employers that comply with the PEL are not subject to exposure assessment. Construction industry employers should focus their efforts on the exposure control methods. The exposure control methods are defined in Table 1 of the OSHA standard, however, methods not included in the standard should be avoided. If an employer is not properly implementing the control methods OSHA will issue citations.
Have your employees wear a real-time DustCount 8899 – Respirable Dust Monitor – Click Here to Learn More
According to Bloomberg Environmental, a Virginia construction company was issued five citations for respirable crystalline silica violations totaling $304,130. In other words, the fines could be the most substantial fines ever under the new silica standard.
For a full copy of the General Industry FAQ, please see this link -> https://www.osha.gov/dsg/topics/silicacrystalline/generalindustry_info_silica.html
If you are an employer with respirable crystalline silica standard potential issues, you may want to monitor the RFI and provide comments and data to OSHA regarding the standard. Refer to the RFI here ->https://www.reginfo.gov/public/do/eAgendaViewRule?pubId=201804&RIN=1218-AD18

by Linda Rawson | Feb 8, 2019 | Industrial Hygiene
As a result of the new and revised 2017 OSHA regulation for respirable crystalline silica, OSHA has been trying to clear any questions concerning compliance.

Master Sgt. Donnie Bogan saws cutting lines in concrete, licensed under the terms of the United States Government Work.
The controversial crystalline silica guideline from OSHA took effect on June 23, 2016. Industrial sectors had between one and five years to fully comply with the new standard. The building and construction sector’s conformity day was Oct. 23, 2017.
The regulation lowered the Permissible Exposure Limit (PEL) required dust controls as well as safer work techniques and called for employers to offer respirators to employees when other safe job techniques were unable to restrict respirable crystalline dust exposure.
Employers need to evaluate the exposure of each worker that is or may reasonably be anticipated to be subjected to respirable crystalline silica at or above the authorized limit making use of either an efficiency alternative or a set up monitoring option.
According to Bloomberg Environmental, a Virginia construction company was issued five citations for crystalline silica violations totaling $304,130 USD. The fines could be the largest fines ever under the new silica standard.
Recently, OSHA released a brand-new silica standard Frequently Asked Question (FAQ) to offer some clarification. The new FAQs were created after talking to the general industry and industry stakeholders.
The goal of the new silica standard FAQ is to give further guidance to both companies and employees on the silica standard’s requirements. The areas highlighted are methods of compliance, exposure assessments, regulated areas, and communication of respirable silica hazards to employees.
Here are three frequently asked questions published in the OSHA General Industry FAQ.
Q: Can employers use data from real-time monitoring and exposure mapping to assess employee exposures under the performance option?
A: Yes. Data generated by real-time monitoring of respirable dust levels (conducted using direct-reading instruments) can be combined with exposure mapping to assess employee exposures under the performance option, provided that the data can be correlated with individual employee exposures and otherwise meet the requirements for objective data. OSHA notes that in order to estimate the level of respirable crystalline silica in the air using real-time monitoring data, employers must also know the percentage of silica in the dust (e.g., from the analysis of a bulk sample or information from a safety data sheet). If an employer does not know the percentage of silica in the dust, it can assume 100% of the respirable dust is silica for purposes of determining worst case exposures from real-time monitoring data under the standard.
Q: If an employer characterizes employee exposures under the performance option using objective data from real-time monitoring and exposure mapping, how often does the employer need to repeat the monitoring and mapping process?
A: The goal of the performance option is to give employers flexibility to accurately characterize employee exposures using whatever combination of air monitoring data or objective data is most appropriate for their circumstances. Therefore, OSHA has not specified exactly how often data should be collected for these purposes. Employers may rely on existing data as long as the data continues to be sufficient to accurately characterize employee exposures. OSHA notes, however, that accurately characterizing employee exposures is an ongoing duty, and employers must reassess exposures whenever a change in the production, process, control equipment, personnel, or work practices may reasonably be expected to result in new or additional exposures at or above the AL, or when the employer has any reason to believe that new or additional exposures at or above the AL have occurred. See 29 C.F.R. § 1910.1053(d)(4)
Q: If personal sampling results show that one employee, who works in a small, non-enclosed area of a large building, is exposed above the PEL, but another employee, who is only a short distance away, is exposed below the PEL, how does the employer decide how far to extend the regulated area?
A: Because there is an exposure above the PEL, the facility must determine which task or operation is creating the overexposure and create a regulated area around that task or operation. In the example provided, the regulated area may include only the first employee’s work station. If the second employee is not exposed above the PEL and is not reasonably expected to be exposed above the PEL, the regulated area does not have to cover that employee’s work area. An employer could choose to use area sampling, real-time monitoring, or exposure mapping to assist in identifying the boundaries of a regulated area.
For a full copy of the General Industry FAQ please see this link -> https://www.osha.gov/dsg/topics/silicacrystalline/generalindustry_info_silica.html

